Secondary and superior cleft sign
Injuries that occur immediately near the pubic bone
The cleft signs are injuries that occur immediately near the pubic bone, the symptoms of which are often mistaken for those of osteitis pubis but which have little to do with this inflammatory process.
As the symptoms associated with the cleft signs resemble those associated with osteitis pubis, adductor tendonitis as well as ‘sports hernia’, these conditions should be ruled out before starting therapy.
In the case of a cleft syndrome injury, a narrow gap forms between the pubic bone, the adductor muscles that attach there, and the rectus abdominis muscles. This means that the insertion of the adductor muscles, particularly the adductor longus muscle, has become slightly detached from the pubic bone and is therefore no longer properly anchored there. Strain on the adductor muscles or rectus abdominis then triggers pain in the bone and muscles, or in the groin region.
The superior cleft and secondary cleft signs differ only in terms of the region where the cleft between the bone and the musculature occurs.
The causes of this cleft syndrome, which manifests as load-dependent adductor and groin pain, have not yet been definitively determined. Possible causes include instability (macro- and microinstability) of the pubic symphysis, chronic overload of the adductor muscles with increased tensile stress at the bony insertion, hip joint diseases with their biomechanical effects on the anterior pelvic ring, and even acute injuries following a fall onto the pelvis.
Diagnosis
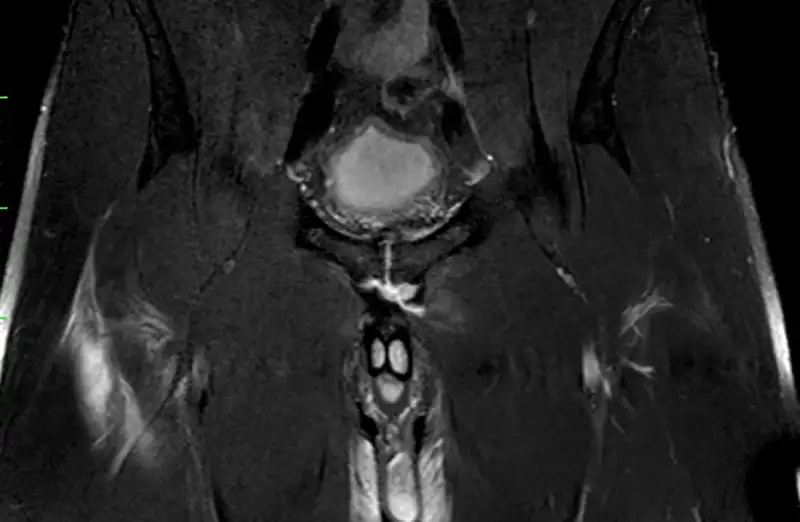

Along with a thorough examination of the patient and the typical pain triggers in the adductor musculature near the pubic bone, which occasionally radiates to the opposite side, cleft signs are confirmed using MRI.
In addition, it is often useful to perform a symphysiograph. This X-ray or CT-based examination can determine the extent of the cleft syndrome and its precise location. Cleft syndromes are classified into PLACT 1–PLACT 6 depending on the severity of the injury and the anatomical structures involved. Based on the severity of the injury visible on the MRI, treatment can be planned with the patient.
Therapy
Therapy for cleft signs has not yet been fully verified and only promises limited success.
Along with targeted injections into the pubic bone cleft with solutions containing cortisone, hyaluronic acid or ACP, there is also the option of surgical treatment. If there has been no improvement with non-surgical treatment (rest, injection and physiotherapy), an option for performance-oriented athletes is surgery, which I have been performing for many years. The aim of the operation is to close the defect between the bone and the musculature.

The results of surgical treatment of cleft palate are good, especially considering the long periods of absence patients experience prior to diagnosis. After surgical treatment of cleft palate, patients should expect a return to sport period of approximately 3-6 months.